Osteomyelitis
As a benign-appearing lytic lesion¶
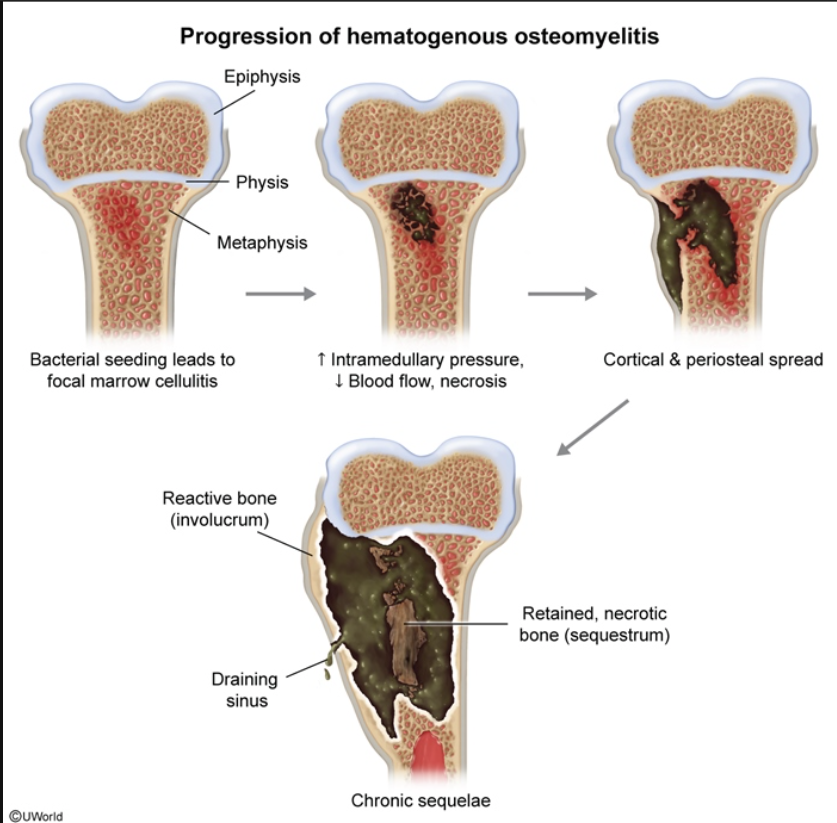
- When bony sequestrum is seen, OM should be strongly considered
- Only lesions that demonstrate sequestra are infection, Eosinophilic granuloma, lymphoma, and fibrosarcoma
Discriminators¶
None
- Fever, back pain, focal spinal tenderness after UTI suggests vertebral osteomyelitis most likely hematogenous spread
- Fever present in <50% of cases
- Exquisite focal tenderness at spinous process; muscle spasm in contiguous area and decreased ROM
- Epidural abscess may result if infection extends posteriorly into epidural space
- Workup is CBC, blood culture, ESR/CRP
- Leukocytes may be normal but ESR/CRB usually elevated
- X-ray may show vertebral collapse but often normal in early osteo
- MRI is imaging modality of choice
- Radionucleotide bone scan w/ gallium is alternate for pts that can't do MRI
- CT-guided aspiration and culture of infected intervertebral disc space or bone needed to confirm the dx
See: